Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis

 ,
,  ,
, 



Abstract
:1. Introduction
2. Methods
2.1. Searching Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
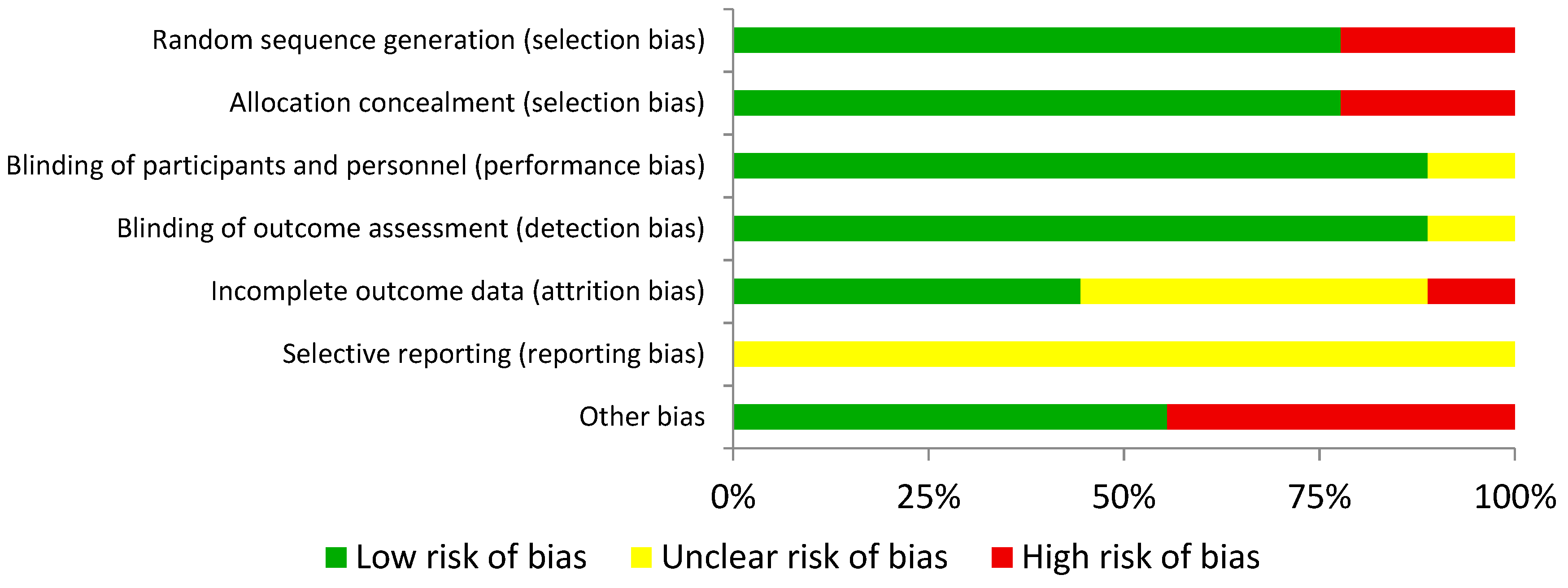
2.4. Quality Assessment of the Experiments
2.5. Statistical Analysis
3. Results
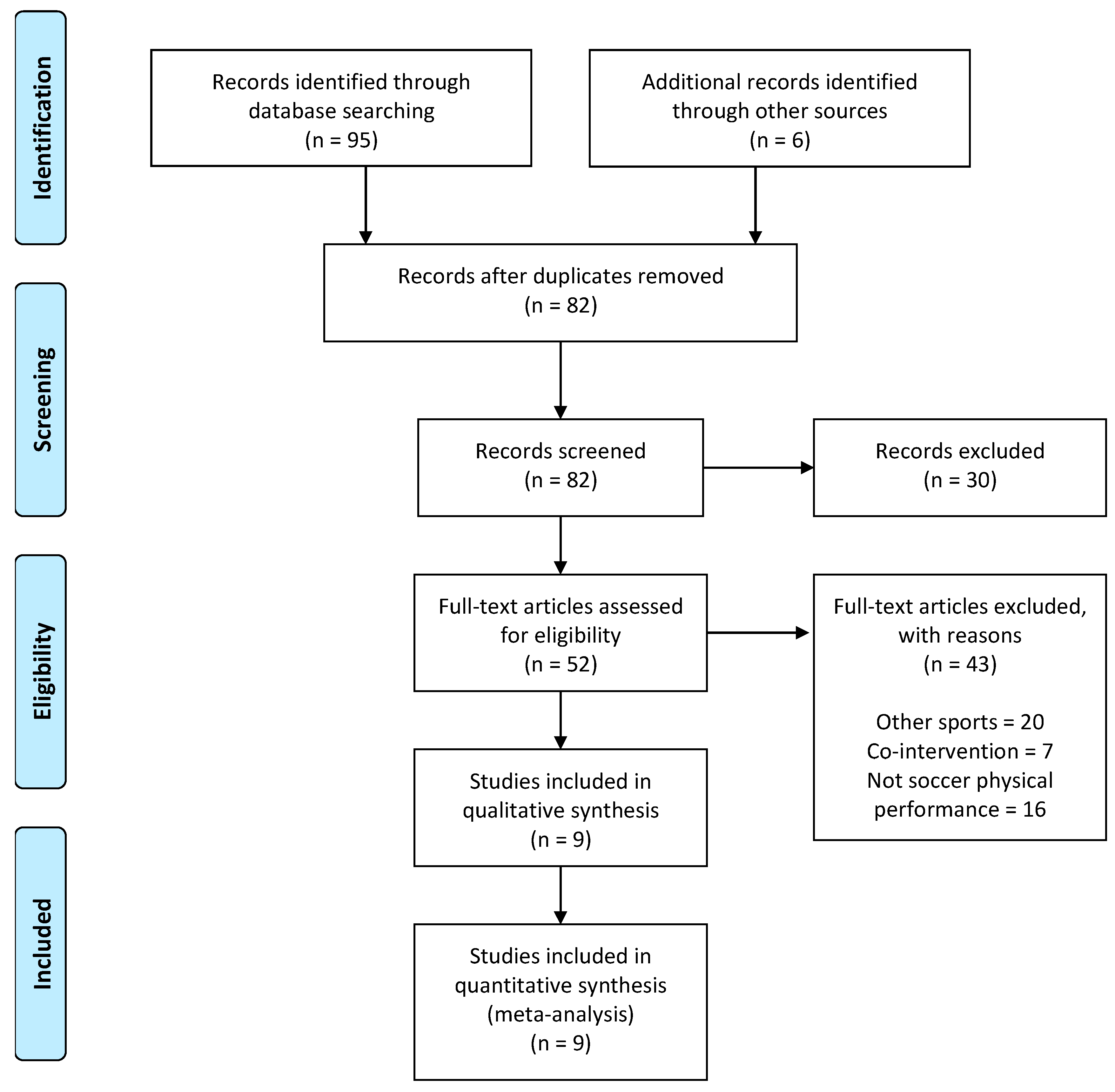
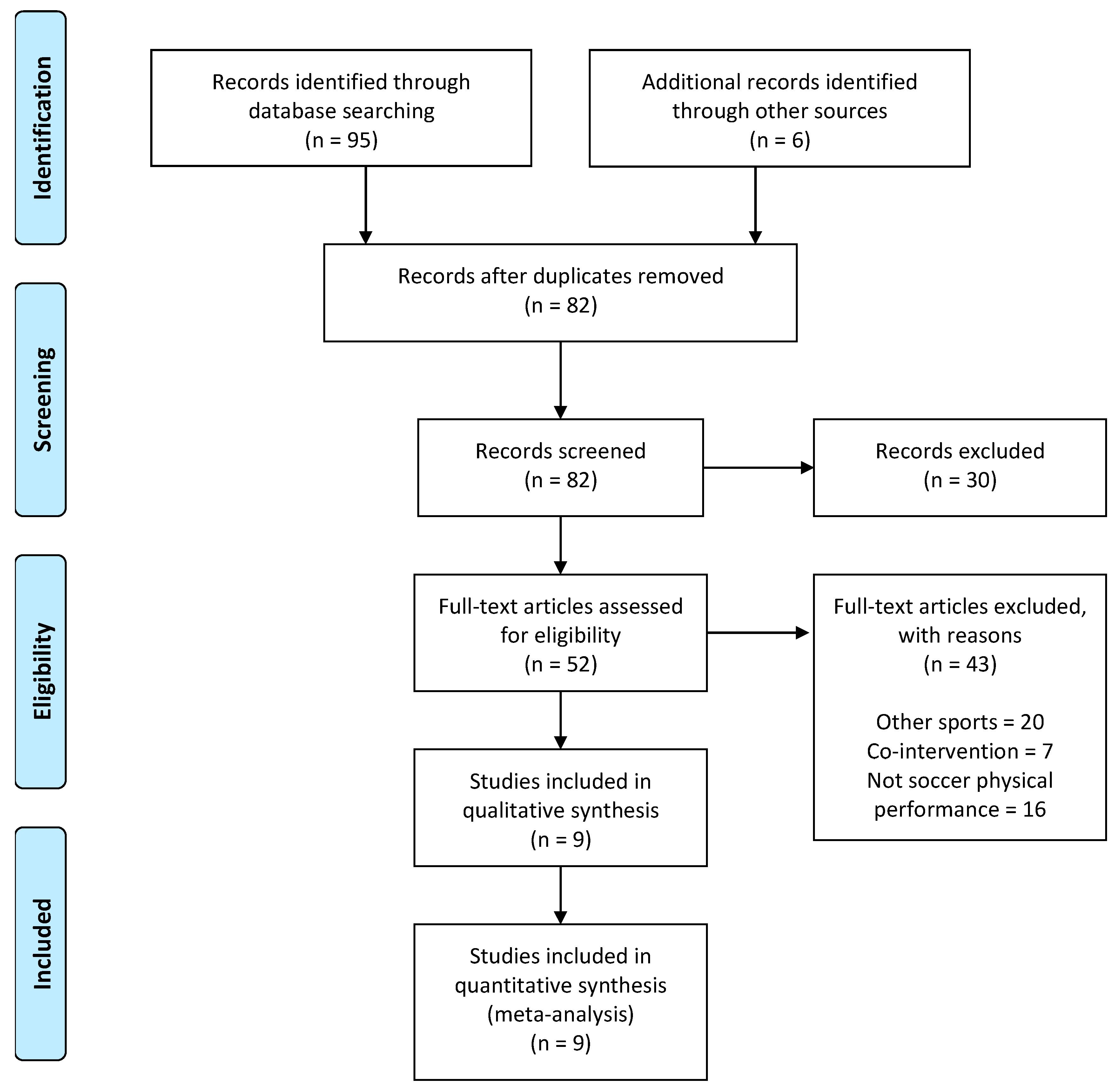
3.1. Main Search
3.2. Creatine Supplementation
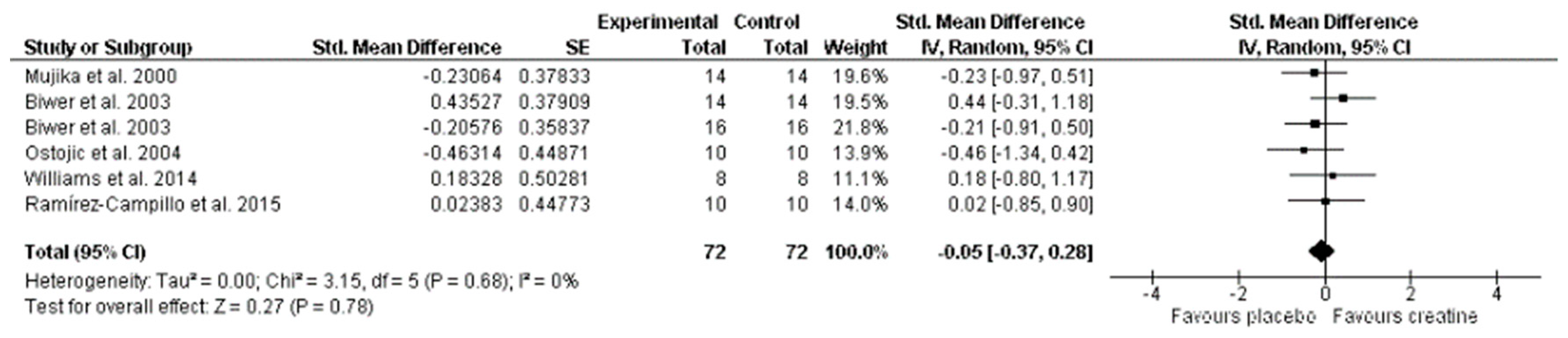
3.3. Effect on Aerobic Performance Meta-Analysis
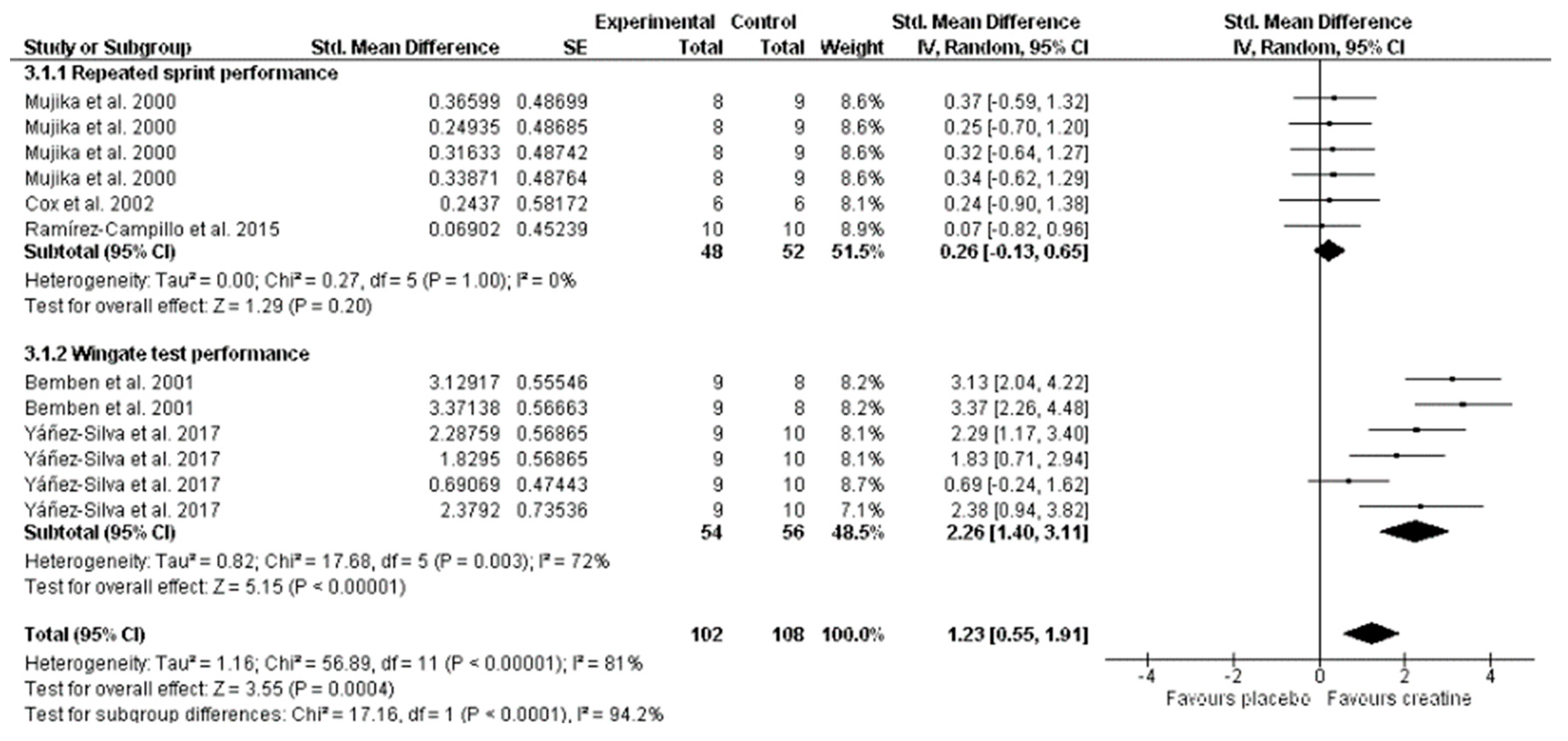
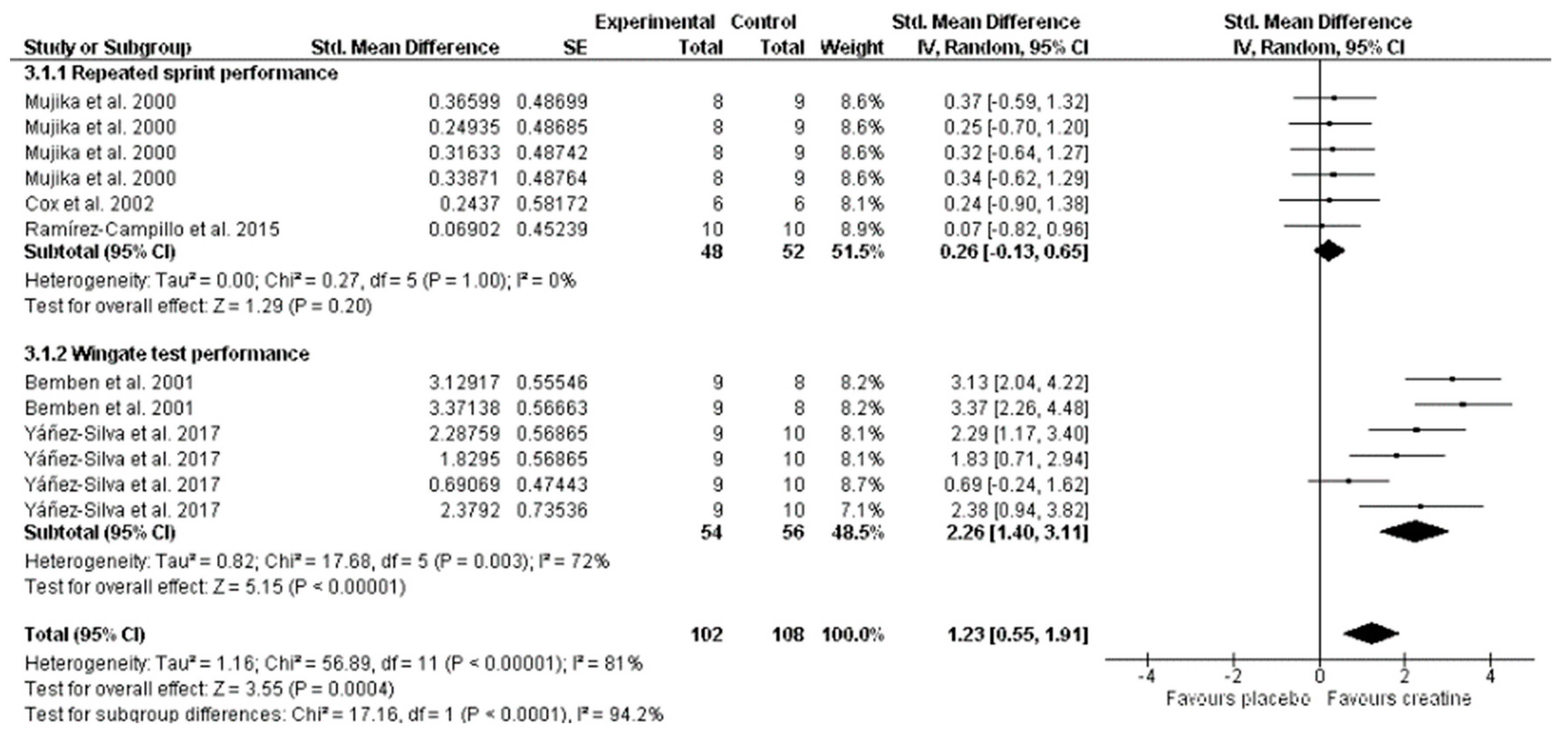
3.4. Effect on Phosphagen Metabolism Performance Meta-Analysis
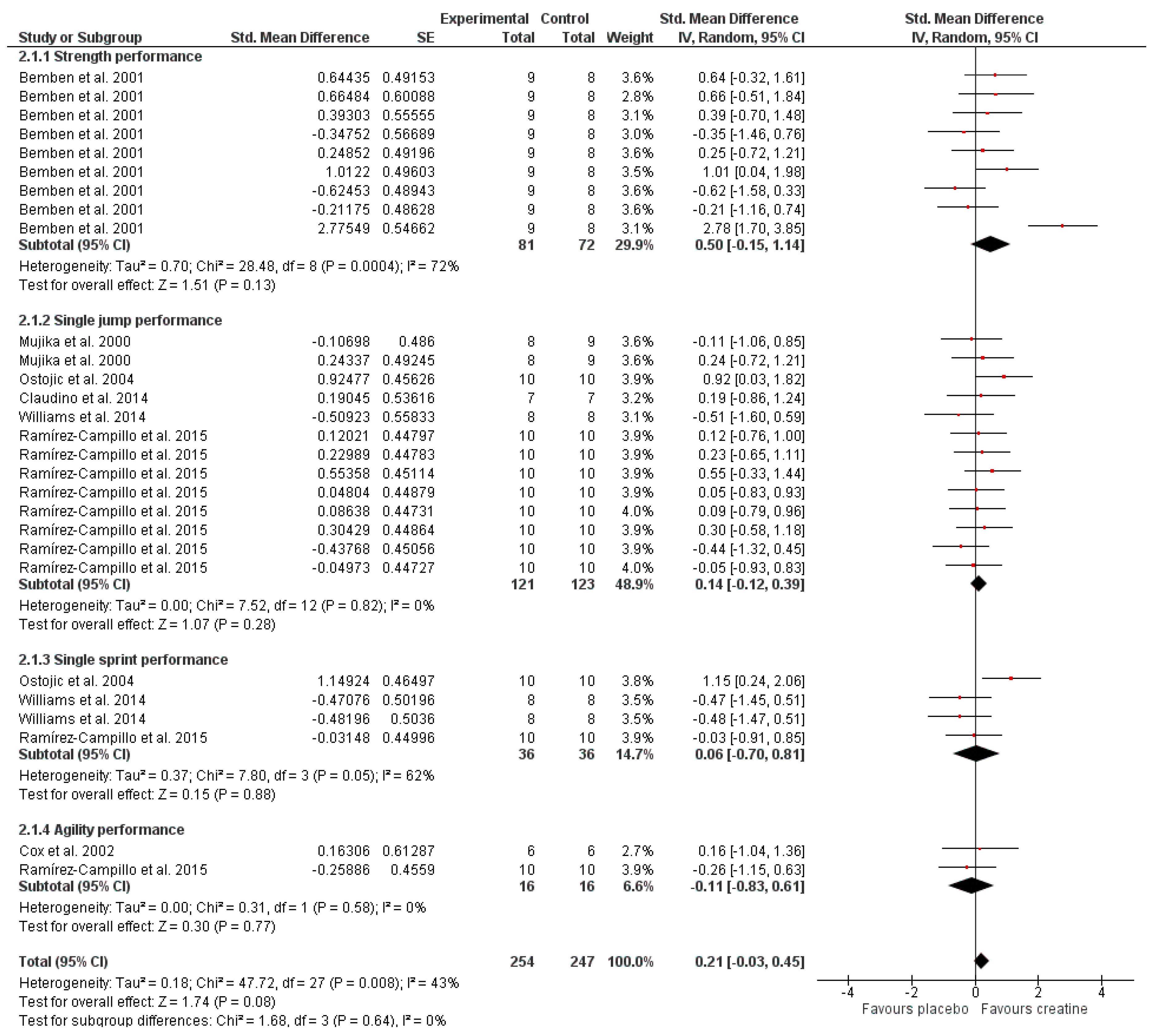
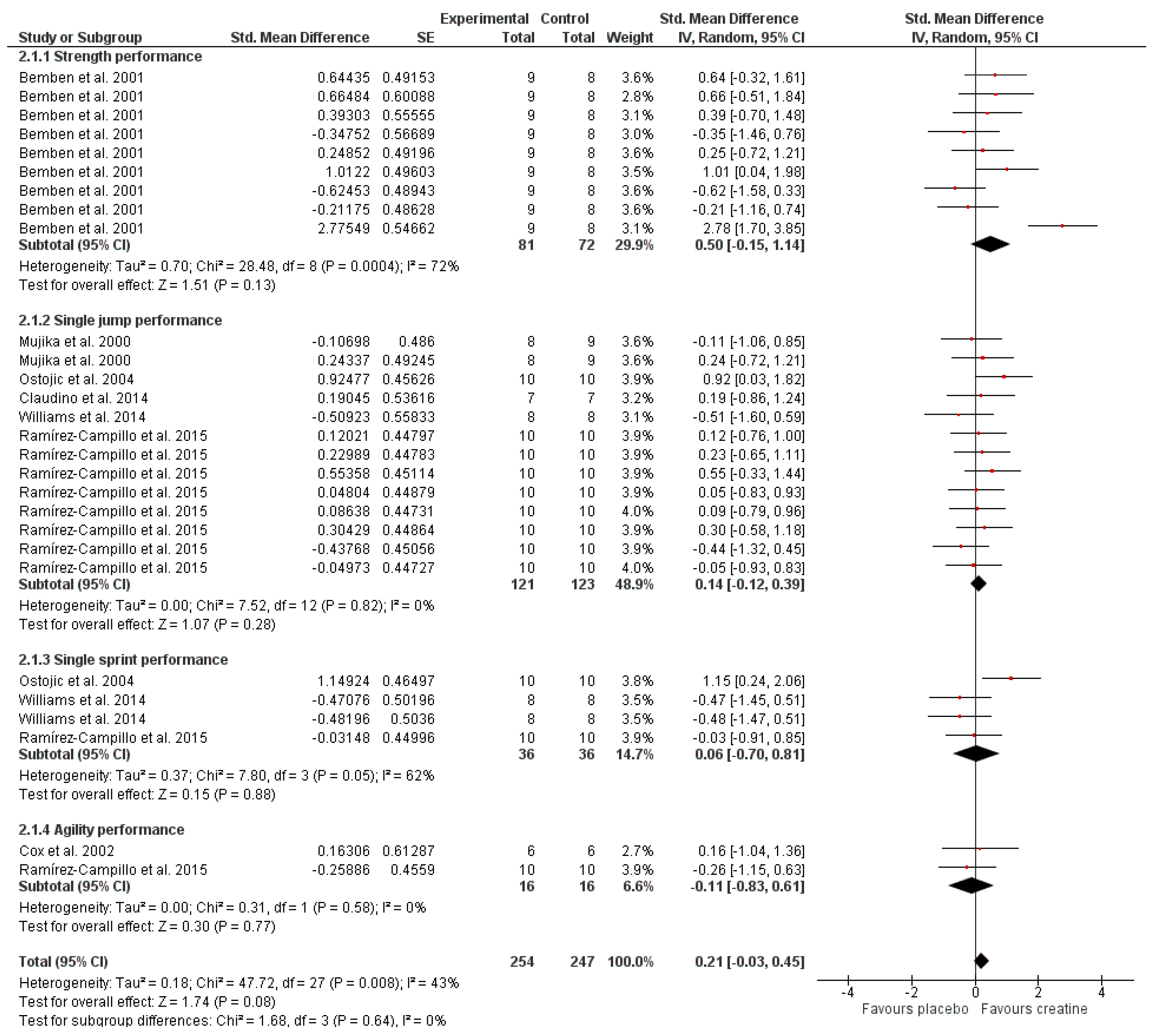
3.5. Effect on Anaerobic Performance Meta-Analysis
4. Discussion
4.1. Effect on Aerobic Performance
4.2. Effect on Phosphagen Metabolism Performance
4.3. Effect on Anaerobic Performance
4.4. Strengths, Limitations, and Future Lines of Research
4.5. Practical Applications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hall, M.; Trojian, T.H. Creatine Supplementation. Curr. Sports Med. Rep. 2013, 12, 240–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, J.S.; McCormick, M.C.; Robergs, R.A. Interaction among Skeletal Muscle Metabolic Energy Systems during Intense Exercise. J. Nutr. Metab. 2010, 2010, 905612. [Google Scholar] [CrossRef]
- Burke, D.G.; Chilibeck, P.D.; Parise, G.; Candow, D.G.; Mahoney, D.; Tarnopolsky, M. Effect of Creatine and Weight Training on Muscle Creatine and Performance in Vegetarians. Med. Sci. Sports Exerc. 2003, 35, 1946–1955. [Google Scholar] [CrossRef] [Green Version]
- Green, A.L.; Hultman, E.; Macdonald, I.A.; Sewell, D.A.; Greenhaff, P.L. Carbohydrate Ingestion Augments Skeletal Muscle Creatine Accumulation during Creatine Supplementation in Humans. Am. J. Physiol. 1996, 271, E821–E826. [Google Scholar] [CrossRef]
- van Loon, L.J.; Murphy, R.; Oosterlaar, A.M.; Cameron-Smith, D.; Hargreaves, M.; Wagenmakers, A.J.; Snow, R. Creatine Supplementation Increases Glycogen Storage but Not GLUT-4 Expression in Human Skeletal Muscle. Clin. Sci. (Lond.) 2004, 106, 99–106. [Google Scholar] [CrossRef]
- Bemben, M.G.; Bemben, D.A.; Loftiss, D.D.; Knehans, A.W. Creatine Supplementation during Resistance Training in College Football Athletes. Med. Sci. Sports Exerc. 2001, 33, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Yanez-Silva, A.; Buzzachera, C.F.; Picarro, I.D.C.; Januario, R.S.B.; Ferreira, L.H.B.; McAnulty, S.R.; Utter, A.C.; Souza-Junior, T.P. Effect of Low Dose, Short-Term Creatine Supplementation on Muscle Power Output in Elite Youth Soccer Players. J. Int. Soc. Sports Nutr. 2017, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Mujika, I.; Burke, L.M. Nutrition in Team Sports. Ann. Nutr. Metab. 2011, 57, 26–35. [Google Scholar] [CrossRef]
- Haycraft, J.A.; Kovalchik, S.; Pyne, D.B.; Robertson, S. Physical Characteristics of Players within the Australian Football League Participation Pathways: A Systematic Review. Sports Med. Open 2017, 3, 46. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, V.; Baron, R.; González-Haro, C.; Gormasz, C.; Pigozzi, F.; Bachl, N. Sprinting Analysis of Elite Soccer Players during European Champions League and UEFA Cup Matches. J. Sports Sci. 2010, 28, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Mohr, M.; Krustrup, P.; Bangsbo, J. Match Performance of High-Standard Soccer Players with Special Reference to Development of Fatigue. J. Sports Sci. 2003, 21, 519–528. [Google Scholar] [CrossRef]
- Krustrup, P.; Mohr, M.; Ellingsgaard, H.; Bangsbo, J. Physical Demands during an Elite Female Soccer Game: Importance of Training Status. Med. Sci. Sports Exerc. 2005, 37, 1242–1248. [Google Scholar] [CrossRef] [Green Version]
- Krustrup, P.; Mohr, M.; Steensberg, A.; Bencke, J.; Kjaer, M.; Bangsbo, J. Muscle and Blood Metabolites during a Soccer Game: Implications for Sprint Performance. Med. Sci. Sports Exerc. 2006, 38, 1165–1174. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]
- Biwer, C.J.; Jensen, R.L.; Schmidt, W.D.; Watts, P.B. The Effect of Creatine on Treadmill Running with High-Intensity Intervals. J. Strength Cond. Res. 2003, 17, 439–445. [Google Scholar] [PubMed]
- Williams, J.; Abt, G.; Kilding, A.E. Effects of Creatine Monohydrate Supplementation on Simulated Soccer Performance. Int. J. Sports Physiol. Perform. 2014, 9, 503–510. [Google Scholar] [CrossRef]
- Mujika, I.; Padilla, S.; Ibanez, J.; Izquierdo, M.; Gorostiaga, E. Creatine Supplementation and Sprint Performance in Soccer Players. Med. Sci. Sports Exerc. 2000, 32, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, S.M. Creatine Supplementation in Young Soccer Players. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 95–103. [Google Scholar] [CrossRef]
- Ramírez-Campillo, R.; González-Jurado, J.A.; Martínez, C.; Nakamura, F.Y.; Peñailillo, L.; Meylan, C.M.; Caniuqueo, A.; Cañas-Jamet, R.; Moran, J.; Alonso-Martínez, A.M. Effects of Plyometric Training and Creatine Supplementation on Maximal-Intensity Exercise and Endurance in Female Soccer Players. J. Sci. Med. Sport 2016, 19, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Mezencio, B.; Amaral, S.; Zanetti, V.; Benatti, F.; Roschel, H.; Gualano, B.; Amadio, A.C.; Serrao, J.C. Creatine Monohydrate Supplementation on Lower-Limb Muscle Power in Brazilian Elite Soccer Players. J. Int. Soc. Sports Nutr. 2014, 11, 32. [Google Scholar] [CrossRef]
- Cox, G.; Mujika, I.; Tumilty, D.; Burke, L. Acute Creatine Supplementation and Performance during a Field Test Simulating Match Play in Elite Female Soccer Players. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.; Green, S.; Higgins, J.P. Defining the Review Question and Developing Criteria for Including Studies. In Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; Cochrane: London, UK, 2008; pp. 81–94. [Google Scholar]
- Green, S.; Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.2. in The Cochrane Library; Wiley Online Library: Chichester, UK, 2009. [Google Scholar]
- Hedges, L.V. Distribution Theory for Glass’s Estimator of Effect Size and Related Estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge Academic: Abingdon, UK, 1988. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying Heterogeneity in a Meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W.; Kreider, R.B.; Stout, J.R.; Greenwood, M.; Campbell, B.; Spano, M.; Ziegenfuss, T.; Lopez, H.; Landis, J.; Antonio, J. International Society of Sports Nutrition Position Stand: Creatine Supplementation and Exercise. J. Int. Soc. Sports Nutr. 2007, 4, 6. [Google Scholar] [CrossRef]
- Rawson, E.S.; Volek, J.S. Effects of Creatine Supplementation and Resistance Training on Muscle Strength and Weightlifting Performance. J. Strength Cond. Res. 2003, 17, 822–831. [Google Scholar] [PubMed]
- Greenhaff, P.L. Creatine Supplementation: Recent Developments. Br. J. Sports Med. 1996, 30, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Bush, M.; Barnes, C.; Archer, D.T.; Hogg, B.; Bradley, P.S. Evolution of Match Performance Parameters for various Playing Positions in the English Premier League. Hum. Mov. Sci. 2015, 39, 1–11. [Google Scholar] [CrossRef]
- Bradley, P.S.; Sheldon, W.; Wooster, B.; Olsen, P.; Boanas, P.; Krustrup, P. High-Intensity Running in English FA Premier League Soccer Matches. J. Sports Sci. 2009, 27, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.; Archer, D.T.; Hogg, B.; Bush, M.; Bradley, P.S. The Evolution of Physical and Technical Performance Parameters in the English Premier League. Int. J. Sports Med. 2014, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rein, R.; Memmert, D. Big Data and Tactical Analysis in Elite Soccer: Future Challenges and Opportunities for Sports Science. SpringerPlus 2016, 5, 1410. [Google Scholar] [CrossRef]
- Roberts, P.A.; Fox, J.; Peirce, N.; Jones, S.W.; Casey, A.; Greenhaff, P.L. Creatine Ingestion Augments Dietary Carbohydrate Mediated Muscle Glycogen Supercompensation during the Initial 24 H of Recovery Following Prolonged Exhaustive Exercise in Humans. Amino Acids 2016, 48, 1831–1842. [Google Scholar] [CrossRef] [PubMed]
- Butts, J.; Jacobs, B.; Silvis, M. Creatine use in Sports. Sports Health 2018, 10, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Kalapotharakos, V.I.; Ziogas, G.; Tokmakidis, S.P. Seasonal Aerobic Performance Variations in Elite Soccer Players. J. Strength Cond. Res. 2011, 25, 1502–1507. [Google Scholar] [CrossRef]
- Arnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Physical Fitness, Injuries, and Team Performance in Soccer. Med. Sci. Sports Exerc. 2004, 36, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalapotharakos, V.I.; Strimpakos, N.; Vithoulka, I.; Karvounidis, C.; Diamantopoulos, K.; Kapreli, E. Physiological Characteristics of Elite Professional Soccer Teams of Different Ranking. J. Sports Med. Phys. Fit. 2006, 46, 515–519. [Google Scholar]
- Chwalbinska-Moneta, J. Effect of Creatine Supplementation on Aerobic Performance and Anaerobic Capacity in Elite Rowers in the Course of Endurance Training. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.; Constantin-Teodosiu, D.; Howell, S.; Hultman, E.; Greenhaff, P.L. Creatine Ingestion Favorably Affects Performance and Muscle Metabolism during Maximal Exercise in Humans. Am. J. Physiol. 1996, 271, E31–E37. [Google Scholar] [CrossRef] [PubMed]
- Rico-Sanz, J. Creatine Reduces Human Muscle PCr and pH Decrements and P(i) Accumulation during Low-Intensity Exercise. J. Appl. Physiol. (1985) 2000, 88, 1181–1191. [Google Scholar] [CrossRef]
- Vandebuerie, F.; Vanden Eynde, B.; Vandenberghe, K.; Hespel, P. Effect of Creatine Loading on Endurance Capacity and Sprint Power in Cyclists. Int. J. Sports Med. 1998, 19, 490–495. [Google Scholar] [CrossRef]
- Syrotuik, D.G.; Game, A.B.; Gillies, E.M.; Bell, G.J. Effects of Creatine Monohydrate Supplementation during Combined Strength and High Intensity Rowing Training on Performance. Can. J. Appl. Physiol. 2001, 26, 527–542. [Google Scholar] [CrossRef]
- Engelhardt, M.; Neumann, G.; Berbalk, A.; Reuter, I. Creatine Supplementation in Endurance Sports. Med. Sci. Sports Exerc. 1998, 30, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Stroud, M.A.; Holliman, D.; Bell, D.; Green, A.L.; Macdonald, I.A.; Greenhaff, P.L. Effect of Oral Creatine Supplementation on Respiratory Gas Exchange and Blood Lactate Accumulation during Steady-State Incremental Treadmill Exercise and Recovery in Man. Clin. Sci. (Lond.) 1994, 87, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, D.; Da Silva, C.D.; Hill-Haas, S.; Wong, D.P.; Natali, A.J.; De Lima, J.R.; Bara Filho, M.G.; Marins, J.J.; Garcia, E.S.; Karim, C. Heart Rate Monitoring in Soccer: Interest and Limits during Competitive Match Play and Training, Practical Application. J. Strength Cond. Res. 2012, 26, 2890–2906. [Google Scholar] [CrossRef]
- Westerblad, H.; Bruton, J.D.; Katz, A. Skeletal Muscle: Energy Metabolism, Fiber Types, Fatigue and Adaptability. Exp. Cell Res. 2010, 316, 3093–3099. [Google Scholar] [CrossRef] [PubMed]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.; Dutheil, F. Creatine Supplementation and Lower Limb Strength Performance: A Systematic Review and Meta-Analyses. Sports Med. 2015, 45, 1285–1294. [Google Scholar] [CrossRef]
- Hoff, J. Training and Testing Physical Capacities for Elite Soccer Players. J. Sports Sci. 2005, 23, 573–582. [Google Scholar] [CrossRef] [PubMed]
- López-Segovia, M.; Marques, M.; van den Tillaar, R.; González-Badillo, J. Relationships between Vertical Jump and Full Squat Power Outputs with Sprint Times in U21 Soccer Players. J. Hum. Kinet. 2011, 30, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Wisloff, U.; Castagna, C.; Helgerud, J.; Jones, R.; Hoff, J. Strong Correlation of Maximal Squat Strength with Sprint Performance and Vertical Jump Height in Elite Soccer Players. Br. J. Sports Med. 2004, 38, 285–288. [Google Scholar] [CrossRef]
- Martinez-Santos, R.; Castillo, D.; Los Arcos, A. Sprint and Jump Performances do Not Determine the Promotion to Professional Elite Soccer in Spain, 1994–2012. J. Sports Sci. 2016, 34, 2279–2285. [Google Scholar] [CrossRef]
- Stølen, T.; Chamari, K.; Castagna, C.; Wisløff, U. Physiology of Soccer. Sports Med. 2005, 35, 501–536. [Google Scholar] [CrossRef] [PubMed]
- Vanderford, M.L.; Meyers, M.C.; Skelly, W.A.; Stewart, C.C.; Hamilton, K.L. Physiological and Sport-Specific Skill Response of Olympic Youth Soccer Athletes. J. Strength Cond. Res. 2004, 18, 334–342. [Google Scholar] [PubMed]
- Al-Hazzaa, H.M.; Almuzaini, K.S.; Al-Refaee, S.A.; Sulaiman, M.A.; Dafterdar, M.Y.; Al-Ghamedi, A.; Al-Khuraiji, K.N. Aerobic and Anaerobic Power Characteristics of Saudi Elite Soccer Players. J. Sports Med. Phys. Fit. 2001, 41, 54–61. [Google Scholar]
- Meckel, Y.; Machnai, O.; Eliakim, A. Relationship among Repeated Sprint Tests, Aerobic Fitness, and Anaerobic Fitness in Elite Adolescent Soccer Players. J. Strength Cond. Res. 2009, 23, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Plowman, S.A.; Looney, M.A. Reliability and Validity of the Anaerobic Speed Test and the Field Anaerobic Shuttle Test for Measuring Anaerobic Work Capacity in Soccer Players. Meas. Phys. Educ. Exerc. Sci. 2002, 6, 187–205. [Google Scholar] [CrossRef]
- Hazir, T.; Kose, M.G.; Kin-Isler, A. The Validity of Running Anaerobic Sprint Test to Assess Anaerobic Power in Young Soccer Players. Isokinet. Exerc. Sci. 2018, 26, 1–9. [Google Scholar] [CrossRef]
- Pekas, D.; Trajković, N.; Krističević, T. Relation between Fitness Tests and Match Performance in Junior Soccer Players. Sport Sci. 2016, 9, 88–92. [Google Scholar]
- Vasileios, A.; Athanasios, S.; Antonios, S.; Nikos, G.; Giorgos, P. The Increase of VO2 Max Variation and the Specific Biochemical Parameters in Soccer Players After a Pre-Season Training Program. J. Phys. Educ. Sport 2018, 18, 686–694. [Google Scholar]
- Polczyk, M.; Zatoń, M. Effects of Glycolytic-Based Interval Training on Anaerobic Capacity in Soccer Players. Hum. Mov. 2015, 16, 149–162. [Google Scholar] [CrossRef]
- Miny, K.; Burrowes, J.; Jidovtseff, B. Interest of Creatine Supplementation in Soccer. Sci. Sports 2017, 32, 61–72. [Google Scholar] [CrossRef]
- Silva, J.R.; Brito, J.; Akenhead, R.; Nassis, G.P. The Transition Period in Soccer: A Window of Opportunity. Sports Med. 2016, 46, 305–313. [Google Scholar] [CrossRef]
- Jeukendrup, A. A Step Towards Personalized Sports Nutrition: Carbohydrate Intake during Exercise. Sports Med. 2014, 44, 25–33. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
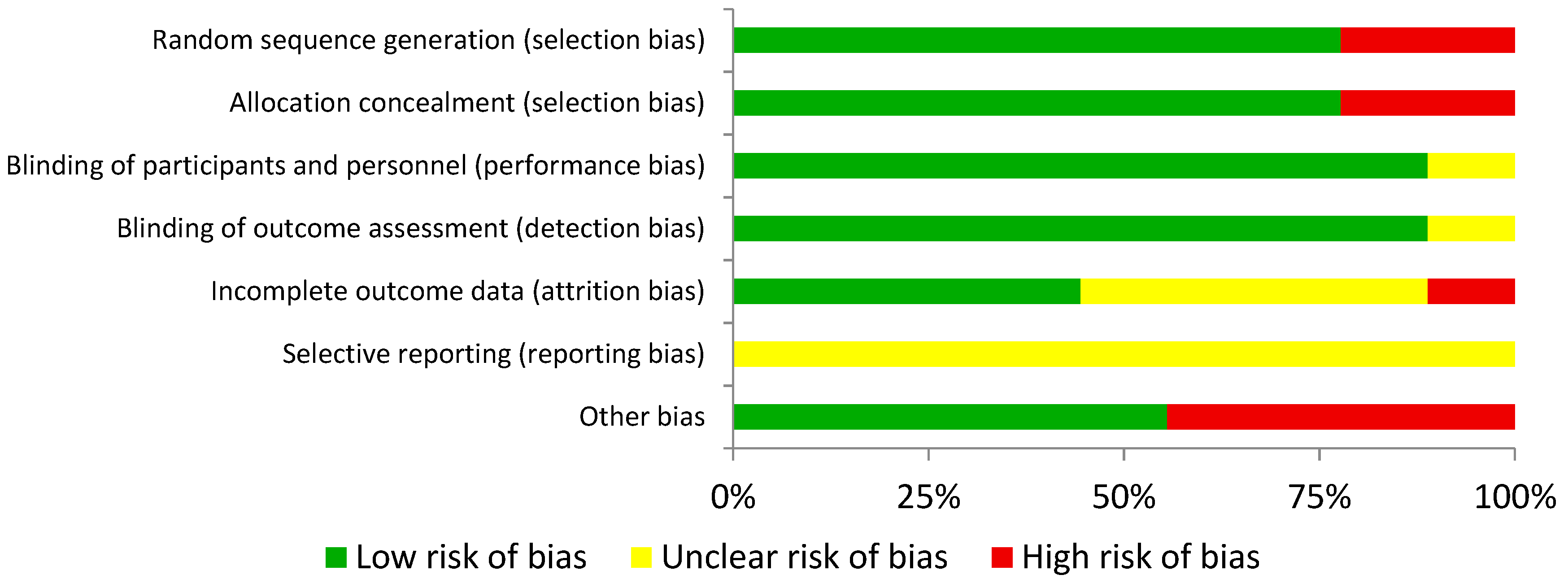
 indicates low risk of bias,
indicates low risk of bias,  indicates unknown risk of bias, and
indicates unknown risk of bias, and  indicates high risk of bias.
indicates low risk of bias, indicates unknown risk of bias, and indicates high risk of bias.
indicates high risk of bias.
indicates low risk of bias, indicates unknown risk of bias, and indicates high risk of bias.| Random sequence generation (selection bias) | Allocation concealment (selection bias) | Blinding of participants and personnel (performance bias) | Blinding of outcome assessment (detection bias) | Incomplete outcome data (attrition bias) | Selective reporting (reporting bias) | Other bias | |
| Mujika et al., 2000 [17] | | | | | | | |
| Bemben et al., 2001 [6] | | | | | | | |
| Cox et al., 2002 [21] | | | | | | | |
| Biwer et al., 2003 [15] | | | | | | | |
| Ostojic 2004 [18] | | | | | | | |
| Claudino et al., 2014 [20] | | | | | | | |
| Williams et al., 2014 [16] | | | | | | | |
| Ramírez-Campillo et al., 2015 [19] | | | | | | | |
| Yáñez-Silva et al., 2017 [7] | | | | | | | |
| Level of participants | Elite | 2 studies [17,21] |
| Semiprofessional or amateur | 7 studies [6,7,15,16,18,19,20] | |
| Age group of participants | Under-17 | 2 studies [7,18] |
| Senior | 7 studies [6,15,16,17,19,20,21] | |
| Type of Cr administration | Based on individual’s body mass | 2 studies [7,15] |
| Absolute dose | 7 studies [6,16,17,18,19,20,21] | |
| Dose used | 30 g/day (3 doses of 10 g daily) | 1 study [18] |
| 20 g/day (4 doses of 5 g daily) | 6 studies [6,16,17,19,20,21] | |
| 0.3 g/kg, four times in one day | 1 study [15] | |
| 0.03 g/kg/day | 1 study [7] | |
| Time of ingestion | Along with breakfast/lunch/dinner or separated by 3–4 h | 5 studies [6,15,16,19,20] |
| Not mentioned | 4 studies [16,17,18,21] | |
| Loading phase | 20 g/day (in 4 doses) for a week plus 1 dose of 5 g/day for 9 weeks | 1 study [6] |
| 20 g/day (in 4 doses) for a week plus 1 dose of 5 g/day for 5 weeks | 1 study [19] | |
| 20 g/day (in 4 doses) for a week plus 1 dose of 5 g/day for 6 weeks | 1 study [20] | |
| No loading phase | 6 studies [7,15,16,17,18,21] | |
| Duration of treatment | 6 days | 3 studies [15,17,21] |
| 7 days | 2 studies [16,18] | |
| 14 days | 1 study [7] | |
| 6 weeks | 1 study [19] | |
| 7 weeks | 1 study [20] | |
| 9 weeks | 1 study [6] |
| AUTHOR/S- YEAR | POPULATION | INTERVENTION | OUTCOMES ANALYZED | MAIN CONCLUSIONS |
|---|---|---|---|---|
| Mujika et al., 2000 [17] | 17 highly trained male players (20.3 ± 1.4 years) |
|
|
|
| Bemben et al., 2001 [6] | 25 male university players (19.3 ± 0.5 years) |
|
|
|
| Cox et al., 2002 [21] | 12 elite female players (22.1 ± 5.4 years) |
|
|
|
| Biwer et al., 2003 [15] | 15 (7 males and 8 females) university players Age not presented |
|
|
|
| Ostojic, 2004 [18] | 20 young male players (16.6 ± 1.9 years) |
|
|
|
| Claudino et al., 2014 [20] | 14 male professional players (18.3 ± 0.9 years) |
|
|
|
| Williams et al., 2014 [16] | 16 amateur male players (26.0 ± 4.5 years) |
|
|
|
| Ramírez-Campillo et al., 2015 [19] | 30 amateur female players (22.9 ± 2.5 years) |
|
|
|
| Yañez-Siva et al., 2017 [7] | 19 young male players (17.0 ± 0.5 years) |
|
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mielgo-Ayuso, J.; Calleja-Gonzalez, J.; Marqués-Jiménez, D.; Caballero-García, A.; Córdova, A.; Fernández-Lázaro, D. Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 757. https://doi.org/10.3390/nu11040757
Mielgo-Ayuso J, Calleja-Gonzalez J, Marqués-Jiménez D, Caballero-García A, Córdova A, Fernández-Lázaro D. Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis. Nutrients. 2019; 11(4):757. https://doi.org/10.3390/nu11040757
Chicago/Turabian StyleMielgo-Ayuso, Juan, Julio Calleja-Gonzalez, Diego Marqués-Jiménez, Alberto Caballero-García, Alfredo Córdova, and Diego Fernández-Lázaro. 2019. "Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis" Nutrients 11, no. 4: 757. https://doi.org/10.3390/nu11040757
APA StyleMielgo-Ayuso, J., Calleja-Gonzalez, J., Marqués-Jiménez, D., Caballero-García, A., Córdova, A., & Fernández-Lázaro, D. (2019). Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis. Nutrients, 11(4), 757. https://doi.org/10.3390/nu11040757